And what is NGSP, IFCC, GMI and eAG?
What is HbA1c? Glucose in the bloodstream will sometimes randomly link (glycate) with a red blood cell’s haemoglobin (Hb) creating “Glycated haemoglobin” or HbA1c. The more glucose there is in the bloodstream the more likely this linking will happen. A red blood cell is in circulation for about 120 days, so the amount of HbA1c in the bloodstream can be used to approximate average blood glucose level over that time.
Diabetics typically have more glucose in their blood, so will have a higher HbA1c. Having a high HbA1c increases the chance of developing negative long term effects of diabetes like retinopathy, amputation or organ failure [cite].
So what is HbA1c? A method to judge how well diabetes is being managed to predict long term health.
The rest of this post is some history, calculations and caveats of HbA1c.Here is an example HbA1c reading from a clinic:
 HbA1c reading from clinic.
HbA1c reading from clinic.
- 49 mmol/mol (IFCC) is the number of HbA1c molecules per 1000 Hb molecules, i.e. 49/1000 or 4.9%
- 6.6% (NGSP aka DCCT) is the same but reported as a percentage
Wait! NGSP is 6.6% and IFCC is 4.9%. So which is correct? The short answer is:
- IFCC (2003) is newer, more accurate measurement, and clinics are moving towards that as the recommended measure.
- NGSP (1996) is older and related to clinical outcomes rather than accuracy.
The conversion is:
NGSP = 0.09148 × IFCC + 2.152 IFCC = 10.93 × NGSP - 23.50
NGSP vs IFCC
Why are these two measurements different?
NGSP (formerly the “National Glycohemoglobin Standardization Program”) was tasked with defining a standard way to report HbA1c after the Diabetes Control and Complications Trial (DCCT) showed in 1993 that:
- HbA1c had a linear relationship with average glucose.
- HbA1c was the highest risk factor for complications of diabetes.
- Lowering HbA1c is worth the risk of potential hypoglycemia. Accepting a high HbA1c (hyperglycemia) was 3x more riskier.
The DCCT involved 1,441 type 1 diabetics for 6 years (1983–1989), and massively impacted the way we manage diabetes today [pdf].
At that time each method, manufacturer and individual machine that measured HbA1c was reporting different results, even from the same blood sample. This made any global HbA1c recommendations impossible.
The NGSP standardised each machine by calibrating them on the same reference values. The values are not 100% accurate, but consistency was the main goal not accuracy. Now advice like “all toddlers should have an HbA1c of less than 7%” is useful no matter where you get your results from.
The International Federation of Clinical Chemistry (IFCC) measurement is more accurate. It doesn’t use a % measurement so it is not confused with NGSP.
HbA1c to Estimated Average Glucose (eAG)
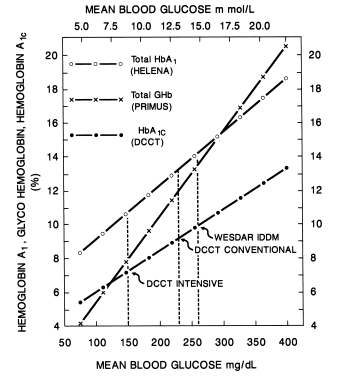
 Relationship shown between HbA1c and Average Glucose from DCCT (1993)
Relationship shown between HbA1c and Average Glucose from DCCT (1993)
It doesn’t really matter if you use IFCC or NGSP, for a diabetic the most useful metric is the estimated average glucose (eAG). Blood Glucose Level (BGL) is the unit a diabetic interacts with every day, so is more readily understood.
Since the DCCT showed a linear relationship between HbA1c and average blood glucose, eAG could be calculated with:
eAG(mg/dl) = 28.7 × NGSP − 46.7 eAG(mmol/l) = 1.59 × NGSP − 2.59
This comes out to a table like:

Or another way to look at it:

What is GMI?
 Example reading from Dexcom Clarity
Example reading from Dexcom Clarity
You can also use average glucose levels to approximate HbA1c, called Glucose Management Indicator (GMI).
Modern Continuous Glucose Meters (CGM) like dexcom G6 give a glucose reading every 5 minutes 24/7. With the mean glucose calculated from the CGM, GMI is calculated with:
GMI(NGSP) = 3.31 + 0.02392 × [mean glucose in mg/dL] GMI(NGSP) = 3.31 + 0.43056 × [mean glucose in mmol/L]
Note: The GMI is only an approximation of HbA1c readings and not 100% accurate, as seen above NGSP is 6.6% where GMI is 6.7%.#### Limitations and caveats of HbA1c?
HbA1c is not enough to predict health. Large spikes and drops in BGL can also increase diabetes complications [cite]. These swings are not visible from the HbA1c alone, as it only calculates the mean value. To show this we need to also use other metrics like time-in-range or standard deviation, both which a CGM can show.
HbA1c readings can also be affected because:
- HbA1c is weighted towards more recent events because not all red blood cells live a full 120 days. So glucose levels for the previous 30 days will impact results more than the levels from 90–120 days.
- HbA1c can be different between people because of sex, age, and/or BMI.
- Chronic illnesses affect HbA1c if they impact red blood cells, e.g. sickle cell anemia red blood cells last only 10–20 days.
- Environment and behaviour affect HbA1c, e.g. inhaled carbon monoxide binds with red blood cells. So smokers, who inhale more carbon monoxide, have higher HbA1c levels. FYI: There is a ton of studies about relationship between smoking an HbA1c [1], [2], [3]
All this means that HbA1c readings are a useful tool to predict long term health for diabetics, but:
- A bad reading is not indicative you are doing badly overall.
- A good reading doesn’t mean that you will have no long term consequences of diabetes.
Links
- Lessons From the Diabetes Control and Complications Trial— JULIO V. SANTIAGO 1993. This is a great article. It explains why HbA1c measurement is the way it is, the research behind it, and I recommend it as a great read about the topic.
- The NGSP website answers a lot of questions about HbA1c here http://www.ngsp.org. The IFCC webpage not so much.
- This article lists a bunch of ways they test for HbA1c